
The knee joint- basic anatomy and function
Introduction

The knee joint is the biggest joint of the human body. It consists of the medial and lateral tibiofemoral and patellofemoral joint.
In contrast to the hip joint the knee joint is predominantly stabilised by ligaments and not osseous structures.
Bony anatomy

The main part of the knee joint (tibiofemoral joint) is bulid by the medial and lateral femoral condyles and the tibial plateau. The tibial plateau is concave on the medial and convex on the lateral side.
The fibula is located at the lateral side of the knee and is connected to the shin bone (tibia) by a tight ligamentous capsule.
In flexion of the knee the knee cap (patella) is guided by the femoral trochlea. From 40° flexion it enters the trochlea and is guided by the osteochondral anatomy.
Ligaments of the knee joint

Collateral ligaments:
The collateral ligaments consist of a medial and lateral one. The medical collateral runs from the medial epicondyle of the thigh (femur) to the medial side of the tibia.
The lateral collateral ligament runs as cord-like structures from the lateral epicondyle to the head of the fibula.
Cruciate ligaments:
One differentiates the anterior from the posterior cruciate ligament. The anterior cruciate ligament (ACL) stabilises the knee in terms of anterior translation. The posterior cruciate ligament (PCL) stabilises the knee in terms of posterior translation. Both act as rotational stabiliser.
Meniscus

The meniscus can be divided in a medial and lateral one. Each meniscus consists of an anterior horn, corpus and posterior horn.
The medical meniscus is connected to the lateral one with a ligament, the transverse ligament.
The function of the menisci cannot be overestimated. The main function is tto stabilised the knee and act as a shock absorber.
Hence it is of utmost importance to save as much meniscus as possible.
Cartilage
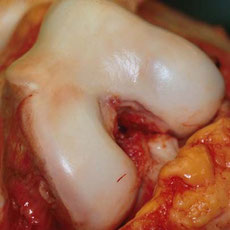
The cartilage covers the knee joint on the articular side.
The function of the cartilage is to reduce friction and facilitate movement of femur, tibia and patella.
Extensor mechanism (e.g. patellar ligaments and quadriceps tendon)

The extensor mechanism consists of the quadriceps tendon, the patellar bone and the patellar tendon.
The force of the quadriceps muscle is transfered by tendons to the bone. Only with an intact extensor mechanism it is possible to straighten our legs.
Neutral leg axis, bowed leg, x-shaped leg

One can differentiate a staight (neutral), from a bowed (varus) and x-shape (valgus) leg:
In a neutrally aligned leg about 60% of the loading forces affect the medial knee joint and only 40% the lateral one.
In the case of a bowed leg up to 80-90% of loading forces affect the medial joint compartment. In a valgus aligned leg more forces go through the lateral compartment.
The resulting chronic overloading on the medial knee compartment in a varus knee can lead to early osteoarthritis.
In such a case an early correction of the leg axis should be performed to avoid early OA.
In the image displayed here shows a patient after leg axis correction ("blue plate"). The novel leg axis is valgus. On the contralateral side remains a bowed leg.